Spine Fracture
On this page, we will try to explain in detail about what is a spinal fracture, what are the types of spinal fractures, its causes and diagnostic methods, surgery and post-operative recovery. I wish you all healthy days.
What is a Spine Fracture?
The spine consists of 33 bones. These bones are connected to each other by soft tissues, joints and cushions between the two spinal bones. The main task of the spine is to ensure that our body stands upright and moves in all directions. It also has a very important task such as protecting the spinal cord in the canal passing through the spine. The spinal cord is responsible for carrying the nerve impulses that come from the brain to the arms, trunk and legs and delivering the responses from those regions to the brain. It loads the strength, sensation and pain function of our arms and legs. In addition, vital functions such as heartbeat and breathing, urine-defecation and sexual functions are among the important tasks.
Spinal fractures are usually seen in the young population as a result of trauma caused by falling from a height or traffic accident. In the elderly, even a simple trauma as a result of bone resorption called osteoporosis can cause a fracture in the spine. In elderly individuals, spinal fractures due to osteoporosis may have a history of low back pain that is sudden and not accompanied by any trauma.
In these patients, the pain increases while standing or walking, while it decreases in the resting state or lying position. If it is not treated, patients may experience a decrease in spinal movements, loss of height in the spine and the resulting pain affects the patient's quality of life very negatively.
Since the fracture that occurs may put pressure on the spinal canal and the missing spinal cord, very important problems leading to paralysis may be encountered in these patients. Traumatized patients need to be transported to the emergency department in the appropriate position, fractures caused by a fall or trauma and compression of the spinal cord may leave the patient paralyzed as a result of improper transportation. Another cause of spinal fractures is a spinal tumor. In these patients, the structure of one or more vertebrae is affected by the tumor, it becomes more vulnerable to traumas and the spine may break even with a very low-energy trauma.80% of patients with spinal fractures are between the ages of 18-50. Men face this problem 4 times more often than women, and most of the fractures occur in the back and waist. Back and lumbar spine fractures are seen in 70%, 5-10% in the neck and the rest in other parts of the spine.80% of patients with spinal fractures are between the ages of 15-50.

Spine Fracture Types
We can classify spinal fractures into two groups as collapse-burst fractures and fractures-dislocations.In collapse-explosion fractures, fracture occurs in the spine as a result of excessive load on the spine with trauma. The type of fracture we see most often is collapse fractures, in which the front part of the spine collapses. If the load on the spine is such that it concerns the front, middle and back part, then we encounter what we call an explosion fracture. In this case, the broken parts can progress to the spinal canal and cause spinal cord injury. In fractured dislocation type spinal fractures, due to the increase in the spine and the load on it, the disc structures, ligaments and joints that hold the spine together are also injured with the fracture, and the connection of the two vertebrae to each other is broken and spinal dislocation occurs. Spinal cord injury can also be seen in this type of fracture. At the same time, the healing times of this type of fractures are long and difficult, surgical treatment is required.

Causes of Spine Fracture
Spinal fractures are mostly caused by high-energy traumas such as falling from a height or a traffic accident in young ages. This type of fracture can occur in osteoporosis without a simple trauma. Spinal fractures due to osteoporosis usually develop suddenly and there is often back or low back pain unaccompanied by trauma. Pain increases while standing or walking in patients, and decreases when resting or when the patient lies on the bed. In patients diagnosed with osteoporosis and not treated, spinal movements are restricted, bone height loss may occur and pain may not go away.
In untreated patients, a hump can occur in the spine as the height of the fractured spine increases further. It is extremely important that patients with suspected spinal fractures are transported to the nearest health institution in a suitable position. Because a fracture that did not cause paralysis, but caused a serious deformity in the spine, may cause paralysis in the patient by pressing on the spinal cord during transportation. Another factor that causes this type of fracture is a spinal tumor. A spinal tumor weakens the bones, and as a result, a fracture of the spine may occur without mild trauma or trauma.
The diagnostic method, which has been seen as the gold standard in recent years, is magnetic resonance imaging. With this examination, it is possible to evaluate the disc structures in the distance between the vertebrae, the regions where the vertebrae articulate with each other, the ligament structures that hold the vertebrae together, the spinal cord and the nerves coming out of it. A decrease in the diameter of the spinal canal below a certain amount in magnetic resonance imaging is considered a sign that the disease has progressed. Electromyography and somatosensory evoked potential tests, which are popularly known as the electrophysiological examination, can evaluate the conduction of the spinal cord and which nerve coming out of the spinal cord is under pressure and to what extent it is affected by this pressure. With this examination method, it is also possible to make a differential diagnosis with other diseases involving the spinal cord.

Spine Fracture Diagnostic Methods
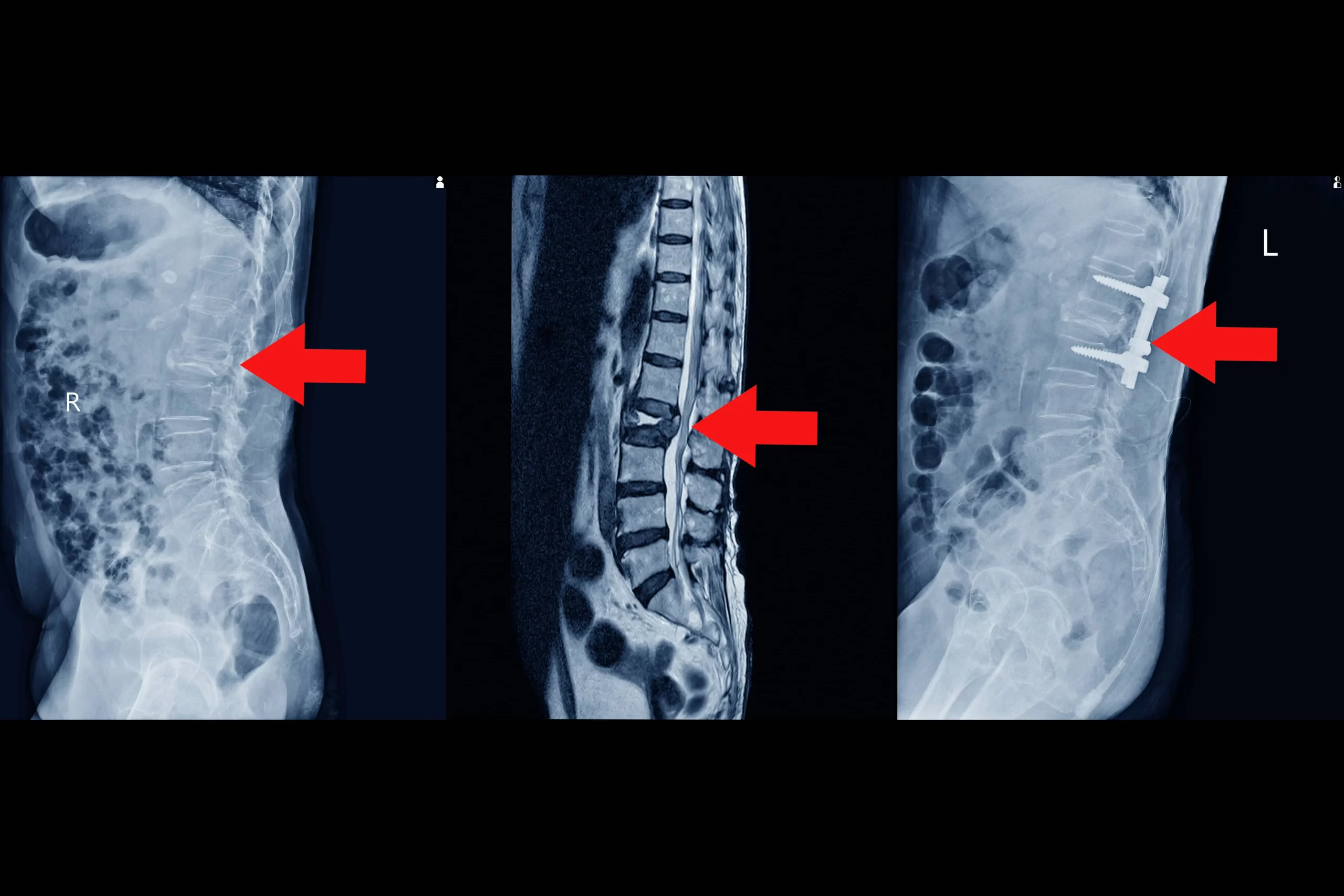
After the patient with a spinal fracture is brought to the hospital, there are procedures that need to be done quickly. The most important of these is to determine whether there is an injury that will affect the vital functions of the patient and to perform the necessary treatment. The patient with a spinal injury should be transported so that the head, trunk and legs are in the same plane for radiological examinations to be performed in the emergency room. The most important of the examinations to be performed in the emergency room is X-ray film, which we call direct radiography. This is the first examination to be performed on patients with suspected spinal injury. Most of the time, it can effectively show us whether there is a spinal injury or not. Patients who are found to have problems in the spine after X-ray filming should be examined with computed tomography for further detailing or patients who do not clearly show a fracture on the X-ray film but are suspected of fracture. In recent years, with the development of technology, the detection and detailing of spinal fractures with computed tomography has become a highly preferred method.
Another method performed with computerized tomography is the examination of spinal fractures with three-dimensional imaging technique. Magnetic resonance imaging is not an imaging method that we prefer when evaluating patients in the emergency room in spinal fractures. However, it can be used to evaluate the severity of the fracture and the condition of the spinal cord and surrounding soft tissues in patients with fractures.
Spinal Fracture Treatment - Spinal Fracture Surgery
In the treatment of spinal injuries, the presence of spinal cord injury and the type of injury are extremely important. The aim of the treatment is to obtain a spine that will not be damaged by the normal loads on the spine and to return the patients to their old life activities in a short time. Usually patients with collapse fractures in the anterior part of the spine are patients whose soft tissues connecting the bones are not affected by this trauma.
They can be treated with simple painkillers or muscle relaxants to be given with bed rest and corset. The use of corsets in our patients helps them to return to their daily work in a shorter time. The duration of using the corset varies between 2 and 4 months depending on the location of the fracture in the spine and the accompanying findings.
Another treatment method used in spinal fractures is surgical treatment. It is the process of detecting the broken spine or vertebrae with metal tools containing titanium or freezing them. Mostly this surgery is applied to patients from the back side. But sometimes it can also be done from the side and front. With the grafts used with titanium-containing metal implants during surgery, the fixation process of the spine can be ensured to remain for many years. The fixation process called fusion can take months to complete. For this reason, patients should be under the control of a neurosurgeon at regular intervals. During this surgery, what we also call decompression, that is, the bone parts that put pressure on the spinal cord or are stuck due to spinal cord injury are cleaned. Decompression and fusion method is used in explosion fractures in which only posterior connective tissues are injured and in other explosion fractures accompanied by neurological injury, and in patients with dislocation with fracture.
In early collapse fractures of the spine, if the anterior height of the spine has not decreased by more than 50% and there is no problem in the posterior connective tissues of the spine, a surgical method called vertebroplasty or kyphoplasty, which is more comfortable for the patient, can be selected. This surgery is usually performed under local anesthesia. A small incision in the skin is made to the spine and a substance called bone cement is injected into the spine with large-diameter needles.
After the proper distribution of this substance in the spine, its freezing is constantly controlled by taking X-ray films and the spine is prevented from collapsing further. In the method called kyphoplasty, bone cement is injected into the spine. However, the difference of this method from vertebroplasty is that before the bone cement is sent, a large-diameter needle with a balloon at the end is entered into the spine and the balloon is inflated, reducing the collapse a little, that is, bringing it to a level close to the old height of the spine. Then, bone cement is injected into the area opened by the balloon as much as the volume of the balloon. Thus, both the spine is strengthened and the loss of height of the spine is significantly corrected.

Recovery After Spine Fracture Surgery
Our patients who have spine fracture surgery with vertebroplasty or kyphoplasty method are carried out by lifting them from bed with a corset 4 hours after the operation on the same day and discharged the next day. Our patients who have undergone surgery with the open surgery technique, which we call fusion and decompression method, stay in the hospital for 2 to 4 days and are lifted up with a corset the next day of surgery.
If there are drains in the operation area, they are withdrawn on the 3rd day at the latest. Patients are discharged after X-ray of the spine is checked. Patients who have undergone surgery can go out of the house in a controlled manner to take short walks after about 20 days of rest at home. After 1 month, they can drive in the city. However, during their walk, they must wear the corset given to them when they are discharged. Corset allows our patients to face less low back pain problems. Our patients are started to have light body exercises after 2 months. However, after 1 month, patients can walk as much as they want and swim to do sports or cool off.
Our patients, whose surgery is performed with fusion and decompression methods, can use public transportation from the end of the second month, and they can continue their normal daily lives without restriction after approximately four months. Our patients can run after 6 months, do personal sports and ride bicycles without being for competition purposes. Patients who have completed 1 year after surgery can do all sports except combat sports and danger sports by obtaining the approval of their physicians who perform the surgery in their routine controls.